High-Risk Early-Stage Triple-Negative Breast Cancer (TNBC)
KEYNOTE-522: Study Design, Efficacy, and Safety Data
KEYNOTE-522: Inclusion & Exclusion Criteria
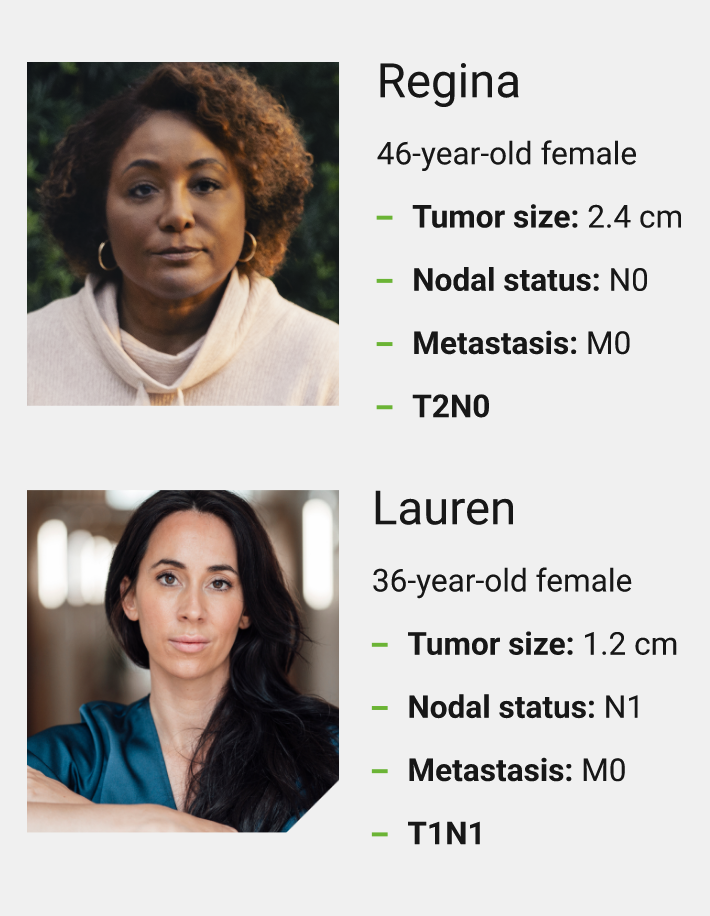
Tumor Size and Nodal Involvement
- >1 cm but ≤2 cm with nodal involvement (N+)
- >2 cm regardless of nodal involvement (N+ or N-)
Key Inclusion Criteria
- Newly diagnosed, previously untreated high-risk early-stage TNBC
- Enrollment regardless of tumor PD-L1 expression
- Tumor size >1 cm but ≤2 cm in diameter with nodal involvement or tumor size >2 cm in diameter regardless of nodal involvement
Key Exclusion Criteria
- Active autoimmune disease that required systemic therapy within 2 years of treatment
- A medical condition that required immunosuppression
N+ = nodal positive; N- = nodal negative; PD-L1 = programmed death ligand 1.
KEYTRUDA is an anti–PD-1 indicated as part of a complete regimen for patients with high-risk early-stage TNBC. Tumor PD-L1 expression is not required for these patients to receive this regimen. If eligible, KEYTRUDA is given in combination with chemotherapy as neoadjuvant treatment and then continued as a single agent as adjuvant treatment after surgery.
Mara Hofherr, PharmD
Oncology Clinical Pharmacist
Delbert Day Cancer Institute
St. Louis, MO
KEYNOTE-522: Study Design
1,174 Patients With Newly Diagnosed, Previously Untreated High-Risk Early-Stage TNBC Were Evaluated in a Randomized, Multicenter, Double-Blind, Placebo-Controlled Trial

Main Efficacy Outcomes
- Pathological complete response (pCR): Defined as absence of invasive cancer in the breast and lymph nodes (ypT0/Tis ypN0) and was assessed by the blinded local pathologist at the time of definitive surgery
- Event-free survival (EFS): Defined as the time from randomization to the first occurrence of any of the following events: progression of disease that precludes definitive surgery, local or distant recurrence, second primary malignancy, or death due to any cause
Additional Efficacy Outcome
- Overall survival (OS): Defined as the time from randomization to death from any cause1
Randomization was stratified by nodal status (positive vs negative), tumor size (T1/T2 vs T3/T4), and choice of carboplatin (Q3W vs weekly).
The trial was not designed to isolate the effect of KEYTRUDA in each phase (neoadjuvant or adjuvant) of treatment.
All study medications were administered intravenously.
Q3W = every 3 weeks; AUC = area under the curve.
Characteristics of Patients From KEYNOTE-522

ECOG PS = Eastern Cooperative Oncology Group performance status.
I was pleased to see that in KEYNOTE-522, patients with high-risk early-stage TNBC who had tumors greater than 2 cm, regardless of nodal involvement, were eligible for participation.
Cynthia Ma, MD
Professor of Medicine
Washington University
St. Louis, MO
KEYNOTE-522: Pathological Complete Response (pCR) Rate
pCR With KEYTRUDA + Chemotherapya vs Placebo + Chemotherapya in the Neoadjuvant Setting

- pCR was defined as the absence of invasive cancer in the breast and lymph nodes (ypT0/Tis ypN0) and was assessed by the blinded local pathologist at the time of definitive surgery
Carboplatin/paclitaxel followed by AC or EC.
Based on the entire intention-to-treat population (N=1,174) patients.
Based on a pre-specified pCR interim analysis in patients (n=602), the pCR rate difference was statistically significant (P=0.00055 compared to a significance level of 0.003).
Based on Miettinen and Numinen method stratified by nodal status, tumor size, and choice of carboplatin.
Superior EFS With KEYTRUDA + Chemotherapya/KEYTRUDA vs Placebo + Chemotherapya/Placebo at IA42
Kaplan-Meier Estimates of EFSb

- 37% reduction in the risk of an EFS eventb with KEYTRUDA + chemotherapya/KEYTRUDA vs placebo + chemotherapya/placebo (HRc=0.63; 95% CI, 0.48–0.82); Pd,e=0.00031
- The number of patients with an event was 123/784 (16%) with KEYTRUDA + chemotherapya/KEYTRUDA vs 93/390 (24%) with placebo + chemotherapya/placebo
Carboplatin/paclitaxel followed by AC or EC.
EFS was defined as the time from randomization to the first occurrence of any of the following events: progression of disease that precludes definitive surgery, local or distant recurrence, second primary malignancy, or death due to any cause.
HR based on stratified Cox regression model.
P value based on a pre-specified EFS interim analysis (compared to a significance level of 0.0052).
P value based on log-rank test stratified by nodal status, tumor size, and choice of carboplatin.
IA4 = fourth interim analysis; FDA = US Food and Drug Administration.
The data from KEYNOTE-522 help inform treatment decisions for my appropriate patients with high-risk early-stage TNBC. In the study, KEYTRUDA + chemotherapy in the neoadjuvant setting, followed by KEYTRUDA as a single agent in the adjuvant setting exhibited superior results for EFS vs placebo + chemotherapy in the neoadjuvant setting, followed by placebo alone in the adjuvant setting.
Cynthia Ma, MD
Professor of Medicine
Washington University
St. Louis, MO
Superior Overall Survival (OS) With KEYTRUDA + Chemotherapya/KEYTRUDA vs Placebo + Chemotherapya/Placebo at IA7
Kaplan-Meier Estimates of OS

- The number of patients with an event was 115/784 (15%) with KEYTRUDA + chemotherapya/KEYTRUDA vs 85/390 (22%) with placebo + chemotherapya/placebo
- 34% reduction in the risk of death with KEYTRUDA + chemotherapya/KEYTRUDA vs placebo + chemotherapya/placebo (HRb=0.66; 95% CI, 0.50–0.87); Pc,d=0.00150
Carboplatin/paclitaxel followed by AC or EC.
Based on stratified Cox regression model.
Based on log-rank test stratified by nodal status, tumor size, and choice of carboplatin.
Based on pre-specified OS interim analysis (compared to a significance level of 0.0050).
IA7 = seventh interim analysis.
When selecting treatment options for appropriate patients with high-risk early-stage TNBC, I consider overall survival data. In KEYNOTE-522, KEYTRUDA in combination with chemotherapy in the neoadjuvant setting and continued as a single agent in the adjuvant setting demonstrated a statistically significant reduction in the risk of death vs placebo in combination with chemotherapy in the neoadjuvant setting, followed by placebo alone in the adjuvant setting.
Cynthia Ma, MD
Professor of Medicine
Washington University
St. Louis, MO
KEYNOTE-522: Overall Survival (OS) in Select Subgroups at IA73
LIMITATIONS: KEYNOTE-522 was not powered to detect differences in the treatment effect in these subgroups, and no statistical testing was planned for this analysis; therefore, no conclusions can be drawn. Results from exploratory subgroup analyses should be interpreted with caution because of the modest patient numbers and potential imbalances in baseline characteristics within the subgroups.

Carboplatin/paclitaxel followed by AC or EC.
CPS = combined positive score.
The results from KEYNOTE-522 support the use of KEYTRUDA in combination with chemotherapy in the neoadjuvant setting, and then continuing KEYTRUDA as a single agent in the adjuvant setting after surgery for appropriate patients with high-risk early-stage TNBC.
Mara Hofherr, PharmD
Oncology Clinical Pharmacist
Delbert Day Cancer Institute
St. Louis, MO
KEYNOTE-522: Selected Safety Profile
The Safety Investigation of KEYNOTE-522 Included 778 Patients Who Received at Least 1 Dose of KEYTRUDA in Combination With Neoadjuvant Chemotherapya Followed by KEYTRUDA as Adjuvant Treatment After Surgery
The median duration of exposure to KEYTRUDA 200 mg Q3W was 13.3 months (range: 1 day–21.9 months).
- adrenal crisis
- autoimmune encephalitis
- hepatitis
- pneumonia
- pneumonitis
- pulmonary embolism
- sepsis in association with multiple organ dysfunction syndrome and myocardial infarction
- febrile neutropenia (15%)
- pyrexia (3.7%)
- anemia (2.6%)
- neutropenia (2.2%)
Carboplatin/paclitaxel followed by AC or EC.
KEYTRUDA Was Discontinued for Adverse Reactions in 20% of Patients
The most common adverse reactions (≥1%) resulting in permanent discontinuation of KEYTRUDA were:

Adverse Reactions Leading to the Interruption of KEYTRUDA Occurred in 57% of Patients
The most common adverse reactions (≥2%) leading to interruption of KEYTRUDA were:

Adverse Reactions Occurring in ≥20% of Patients Receiving KEYTRUDA
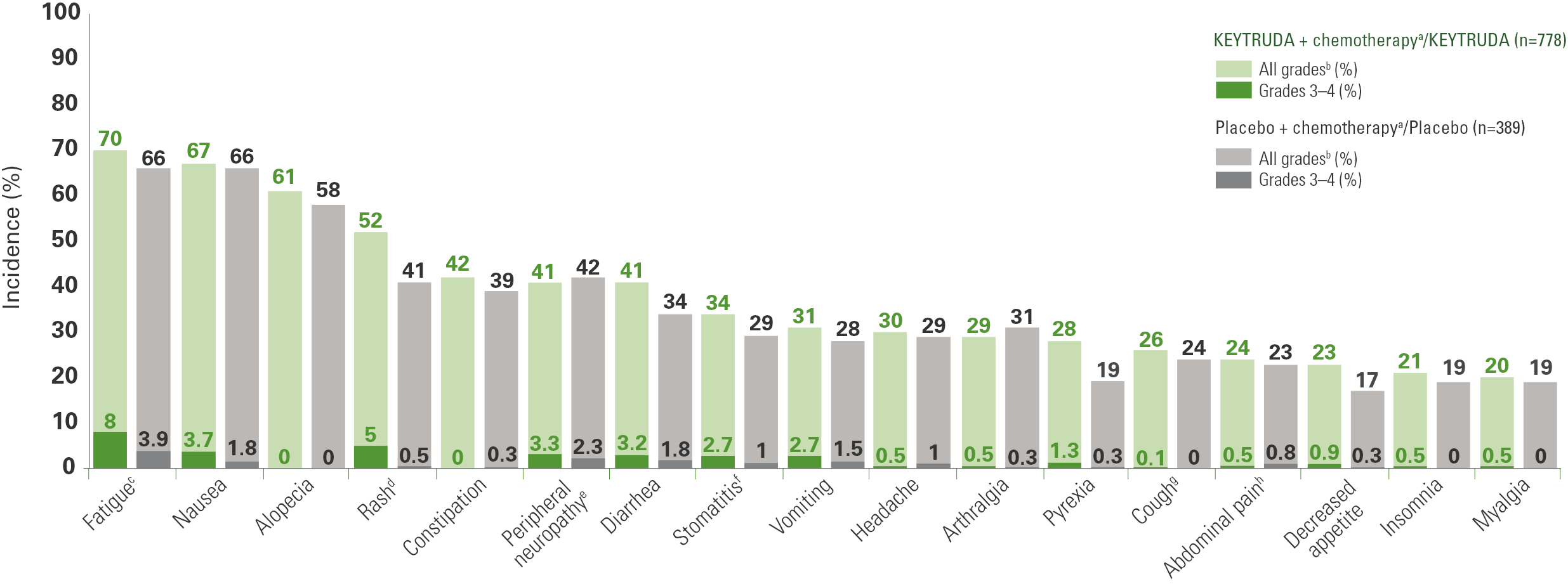
Chemotherapy: carboplatin and paclitaxel followed by doxorubicin or epirubicin and cyclophosphamide.
Graded per NCI CTCAE v4.0.
Includes asthenia, fatigue.
Includes dermatitis, dermatitis acneiform, dermatitis allergic, dermatitis bullous, dermatitis exfoliative generalized, drug eruption, eczema, incision-site rash, injection-site rash, rash, rash erythematous, rash follicular, rash macular, rash maculopapular, rash morbilliform, rash papular, rash pruritic, rash pustular, rash rubelliform, skin exfoliation, skin toxicity, toxic skin eruption, urticaria, vasculitic rash, viral rash.
Includes neuropathy peripheral, peripheral motor neuropathy, peripheral sensorimotor neuropathy, peripheral sensory neuropathy.
Includes aphthous ulcer, cheilitis, lip pain, lip ulceration, mouth ulceration, mucosal inflammation, oral mucosal eruption, oral pain, stomatitis, tongue blistering, tongue ulceration.
Includes cough, productive cough, upper-airway cough syndrome.
Includes abdominal discomfort, abdominal pain, abdominal pain lower, abdominal pain upper, abdominal tenderness.
NCI CTCAE = National Cancer Institute Common Terminology Criteria for Adverse Events.
References: 1. Schmid P, Cortes J, Dent R, et al. Overall survival with pembrolizumab in early-stage triple-negative breast cancer. N Engl J Med. Published online September 15, 2024. doi:10.1056/NEJMoa2409932 2. Schmid P, Cortes J, Dent R, et al; KEYNOTE-522 Investigators. Event-free survival with pembrolizumab in early triple-negative breast cancer. N Engl J Med. 2022;386(6):556–567. doi:10.1056/NEJMoa2112651 3. Schmid P, Cortes J, Dent R, et al. Neoadjuvant pembrolizumab or placebo + chemotherapy followed by adjuvant pembrolizumab or placebo for high-risk early-stage triple-negative breast cancer: overall survival results from the phase 3 KEYNOTE-522 study. Presented at: European Society for Medical Oncology (ESMO) Congress; September 13–17, 2024; Barcelona, Spain.